For decades, a ticking clock has defined the prospects of stroke recovery. In ischemic strokes—which account for 70%–80% of all strokes, the first 4.5 hours after symptom onset are known as the “golden window”, the critical period when treatment is most likely to be effective. But what if patients arrive too late?
A team from the Second Affiliated Hospital of Zhejiang University School of Medicine may have an answer. In a groundbreaking study published on April 3 in The New England Journal of Medicine, researchers led by neurologist Professor LOU Min introduced a new protocol for treating posterior circulation strokes beyond the traditional time limit. Their approach boosted the recovery rate — defined as the proportion of patients symptom-free after 90 days — by a remarkable 53%.

Posterior circulation strokes affect the brainstem, the body’s control hub for vital functions like breathing, heartbeat, and consciousness. Unlike more common anterior strokes, their symptoms can be subtle — such as dizziness, double vision, imbalance — and are therefore often missed or misdiagnosed. The consequences can be devastating: rapid deterioration, coma, or even locked-in syndrome, a condition in which patients are fully conscious but unable to move or speak, communicating only through eye movements.
Intravenous thrombolysis — dissolving the clot with medication to restore blood flow — is the frontline treatment for ischemic strokes. But the current guidelines require it to be administered within 4.5 hours of symptom onset. For many patients, that window closes too soon. In fact, studies suggest fewer than one-third of them arrive at hospitals within this critical time frame.
“There’s a growing gap between treatment guidelines and real-world needs,” said LOU Min. “In many primary hospitals, advanced imaging such as perfusion scans is not available, yet the need for effective treatment is urgent.”
To address this, LOU Min and his colleagues began investigating extended-window intravenous thrombolysis as early as 2009. But the lack of widespread infrastructure and a mature evidence-based research culture delayed large-scale trials. That changed with the establishment of a national stroke big data platform, enabling inter-hospital collaboration and long-term data tracking.
Their two-year clinical trial enrolled patients with posterior circulation strokes who arrived at the hospital between 4.5 and 24 hours after symptom onset. Instead of relying on advanced imaging, the team used a tiered diagnostic approach, starting with clinical symptoms and a standard non-contrast CT scan. The method proved not only practical but also safe: patients who received thrombolysis under this new protocol had a significantly higher recovery rate, with no increase in intracranial hemorrhage or mortality risk.
“By moving away from perfusion imaging and focusing on clinical presentation and basic CT, we’re making treatment more accessible to a broader range of hospitals and patients,” said Dr. YAN Shenqiang, co–first author of the study, alongside Dr. ZHOU Ying.
The implications are profound. The team’s findings challenge the long-standing 4.5-hour treatment limit and offer a viable alternative for patients who cannot undergo mechanical clot removal due to anatomical or logistical reasons.
“This could be a game-changer for stroke care, especially in underserved areas,” said LOU Min. “Patients who missed the golden window now have a second chance.”
Peer reviewers praised the study as “strong evidence that challenges traditional limits of thrombolysis timing,” and noted its potential to reshape clinical guidelines for stroke treatment globally.
For now, the findings offer not only scientific insight but real, renewed hope — that more patients, even those who arrive hours late, might still walk away from a stroke.
Adapted and translated from the article by ZHA Meng
Translator: FANG Fumin
Photo: ZHE Ying
Editor: TIAN Minjie
For decades, a ticking clock has defined the prospects of stroke recovery. In ischemic strokes—which account for 70%–80% of all strokes, the first 4.5 hours after symptom onset are known as the “gold...
ZJU Medicine 7th Issue.pdf
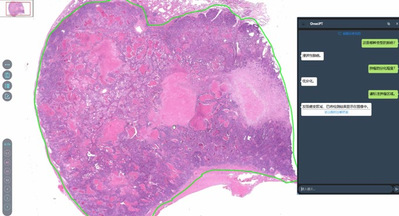
Artificial intelligence (AI)-enabled medical diagnostic tools are improving cancer screening accuracy, helping doctors arrive at more precise diagnoses and enhancing tr...